Does this look like it has been cut deep enough?
I admin a support group on Facebook for parents with tongue-tie babies and this question is often asked. On that group we don’t allow the posting of photos for ‘diagnosis’ or for unqualified opinions by the public because assessment of tongue-tie pre and post division should include as assessment of tongue function and feeding. Photographs can be deceptive as I have seen time and time again.
So how deep do we have to cut to achieve a ‘full’ or ‘adequate’ release? What is a ‘full’ or ‘adequate’ release?
It may come as a shock to those that don’t divide tongue-ties but this question is not that easily answered because there is debate around the world amongst practitioners on how deep is deep enough. I think most people would agree that a division that improves tongue function and feeding is an ‘adequate’ release. But that doesn’t mean to say that in these instances there is going to be ‘full’ and immediate improvement in tongue function and feeding because issues with tongue function and feeding are often more complicated than that. You can do a division which restores normal tongue function but still have ongoing issues with feeding due to a low milk supply as a simple example.
General opinion is that we would normally expect a diamond shaped wound to be achieved. This doesn’t mean that the diamond is always going to be clearly on display whenever the baby opens their mouth. This is because the diamond will only be clearly visible when the tongue is lifted well up into the roof of the mouth. This may occur during strenuous crying or when baby is relaxed and sleeping. Gently and slowly pulling down the lower jaw when baby is in a deep sleep is a good way to visualise the wound. Lifting the tongue gently with your fingers will also expose the diamond. If the tongue is not in an elevated position or is only partially elevated the wound will look linear rather than diamond shaped.
But is the wound always diamond shaped? Well, it depends on how the tissues behave when the tongue-tie is divided and the anatomy of other oral structures. Prominent Wharton’s Ducts (Salivary glands) in the floor of the mouth may make the wound look triangular. Some wounds can look more circular. Very tight tongue-ties or very anterior tongue-ties when divided may split into quite a large diamond due to the tension within the frenulum. Other more posterior or less restrictive tongue-ties may form a more discreet wound. Does the appearance of the wound impact outcomes? Not in my experience and there is certainly no research on this.
Two normal wounds two days after division that look quite different:


The anatomy of the lingual frenulum (a tongue-tie is a restricted lingual frenulum) is complex and will vary from baby to baby. Nikki Mills, an ENT Surgeon from New Zealand published two studies in 2019 which radically changed our understanding on this. It is not a discreet structure and connects to the underside of the tongue and into the floor of the mouth or lower gum. It is a layered structure composed of up to 3 layers- oral mucosa (the thin skin that lines our mouth), fascia and muscle fibres and may be infiltrated by branches of the lingual nerve and small capillaries from the lingual veins. The lingual frenulum is formed from a fold in the mucosa that arises from the floor of the mouth. When the tongue moves this fold will be pulled up from the floor of the mouth. In some tongue-ties only the mucosa is mobilised and these tongue-ties are very thin in appearance, usually divide easily with little bleeding and are likely to be less prone to recurrence as mucosa doesn’t usually form scar tissue. But in a lot of frenulums the layer of fascia that lies beneath the mucosa will be pulled up inside the fold of mucosa. These tongue-ties often look thicker and may feel quite fibrous to cut and when dividing these we often feel a ‘pop’ as the tension releases. This release of tension may create a bigger more prominent wound in some cases. Fascia isn’t vascular so doesn’t usually bleed much but it is more prone to scar formation so these are the tongue-ties where we may see more cases of recurrence. In some cases, not only is the layer of fascia pulled up into the fold of mucosa, but also the fibres of the genioglossus muscle because in some babies these will be suspended close under the layer of fascia. Muscle is vascular and will bleed when cut. But with frenulums that do involve the muscle layer it can be difficult to avoid nicking it and causing some bleeding. Parents as well as practitioners must accept that some babies will bleed more than others and that is down to their anatomy that no one has the power to change. some frenulums will be infiltrated by capillaries (tiny blood vessels) which can be hard to visualise and again may lead to more bleeding.
So, what does this mean in terms of the depth of the cut. When we divide, we are aiming to release the tongue to the extent that is can function better so the baby can feed more effectively. We aren’t aiming for a wound of a certain size or depth. A frenulotomy procedure (division of the tongue-tie) aims to divide the mucosa and fascial layers. We are not trying to divide the muscle layer as that is a different procedure known as a myotomy. According to Nikki Mills, deep divisions risk lingual nerve damage which can lead to loss of sensation in the tongue and impaired function. It may also lead to excessive scarring and as scar tissue isn’t stretchy this is going to cause further restriction in tongue function (recurrence of the tongue-tie). Plus of course if we divide too deep and too wide there is the risk of bleeding from cutting into the muscle layer and cathicng the lingual veins which lie either side of the frenulum. Some tongue-ties have salivary tissue attached through them and we don’t want to cause trauma to this tissue as that can lead to ranula formation which can, in some cases, require surgical repair.
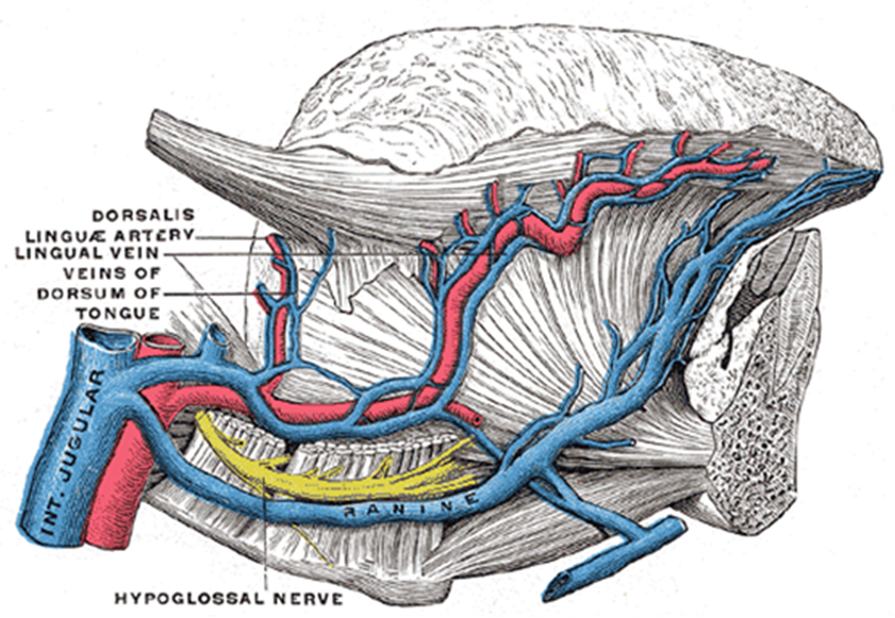
Blood vessels within the mouth. You can see how close to the underside of the tongue the veins are.

{kind=link}
So, tongue-tie practitioners tread a fine line. We need to release deep enough for the baby to achieve better tongue function and feeding but not so deep to cause damage, excessive scar formation and heavy bleeding.
Because a tongue-tie isn’t a discreet structure and connects to the floor of the mouth via the mucosa and fascia (which extends throughout our body) and to other muscles which influence tongue movement division alone is not going to always be sufficient to achieve better tongue function and bodywork may be required. Furthermore, all babies will need to go through a process of adaptation to the extra movement in their tongues and will suffer a degree of muscle fatigue, and may have some low tone initially, so division is not likely to ne the instant fix I certainly wish it was. So, support with feeding, which may include tongue exercises, is going to be required.
A word about laser division. The wounds created with laser will look quite different to those created with scissors because laser vaporises tissue, so the frenulum isn’t simply divided it is removed. The wounds often look deeper and wider than those created with scissors but for all the reasons stated above, aiming for this type of wound is not necessarily desirable because of the risks involved. Plus, data I have collected and hope to present and publish, from a group of 1611 families, suggests that babies who undergo laser division experience more signs of pain and have more difficulty feeding the days after division than those who have scissor division.
When dividing a tongue-tie do we want to be cutting deep into the muscle layer? No. Not just because of the risk of bleeding but because we may also damage the lingual nerve which can cause loss of sensation to the tongue and impair tongue function.
So, when you as a parent, healthcare professional or breastfeeding supporters make accusations around a division not being ‘deep enough’ please stop and think what you are saying and would you be happy with the consequences of a practitioner cutting too deep. it is so very easy when you are not holding the scissors and taking responsibility for the success of that procedure and the safety of that baby to be critical.
Are some tongue-ties not fully divided? Yes certainly. Sometimes this is intentional to avoid the complications already mentioned. (Your practitioner should explain this to you and what further actions needs to be taken). Sometimes accidently because in very small newborns with the tighter tongue-ties it may be difficult to visualise the base of the frenulum. There will be some practitioners who have not been well trained or are inexperienced and this may lead to an ‘inadequate’ release. I also know of some surgeons who are open about the fact that they only divide the anterior part of the frenulum but leave the posterior part intact because they do not believe there is any need to divide it.
If you are worried about your baby’s progress after a division then your first port of call should be the practitioner who did the division. If for any reason you cannot access them, or you don’t feel comfortable going back to them then seek out another experienced tongue-tie practitioner for a second opinion. A directory to assist you is available here https://www.tongue-tie.org.uk/. Your baby and your feeding journey are precious. Please don’t base your decisions and actions on the unqualified opinions and experiences shared by people you have never met over social media.
If we have had a baby with a feeding difficulty related to tongue-tie, we are experts on our own baby and that experience and we can empathise with those families in similar situations. But that does not provide us with the skills and experience that practitioners have who see thousands of babies and support thousands of feeding journeys. Every baby is unique, and support must be tailored to that unique situation. Our personal experiences are never universal and what happened to us, what was helpful to us or what didn’t work for us cannot be applied to everyone else. If we are offering our services as breastfeeding supporters, or indeed healthcare professionals our own personal experiences and feelings should be set aside.
S Oakley 27/8/23
Why is my baby fussing?
All babies will have periods where they are unsettled, cry and ‘fuss.’ This is normal behaviour. Babies don’t have the power of language so they ‘fuss’ to let us know something isn’t right or they need something. Common reasons are overtiredness, too much stimulation, and wanting to be held to feel safe and connected to…
POSTERIOR TONGUE-TIE
I often get enquiries for parents asking me if I cut ‘posterior’ tongue-ties. These parents often do not have a clue what this terminology means as no one has explained it to them. But they are sometimes given the impression division of this type of tongue-tie is complicated and risky. So, this blog will seek…
Myofunctional Therapy and Babies
I deliberately avoided this issue when writing my book ‘Why Tongue-tie Matters’ in 2020/21 because of the lack of evidence and my own conflicting thoughts on this. But I often get asked for my opinion and whether I would advise parents to seek out myofunctional therapy so for what it is worth here is where…
A nipple shield story
Just wanted to share a positive development in our feeding journey. It took 18weeks (15post division) but Edward has suddenly started feeding without nipple shields. I don’t think I believed you and others who said it will likely just happen when he’s ready. I used to try daily, then gave up about a month ago…
Joshua
Hi Sarah, You may not remember me but Autumn 2021 we saw you a couple of times in your clinic (and a couple of times at Ely Milks) with our son Joshua. He had a very severe tongue tie (you said it was probably one of the worst 5 you’ve ever seen), and had to…
A thank you from Naomi and Charlotte
Hi Sarah, I just wanted to give you an update as it has now been about a month since you did my baby Charlotte’s tongue tie division. It took a while to see a big difference, and you said it could, but she now latches a lot better, much reduced clicking and reflux. My supply…