I often get enquiries for parents asking me if I cut ‘posterior’ tongue-ties.
These parents often do not have a clue what this terminology means as no one has explained it to them. But they are sometimes given the impression division of this type of tongue-tie is complicated and risky. So, this blog will seek to address this.
A tongue-tie occurs when the lingual frenulum is too short, and/or tight and/or is attached to close to the tip of the tongue to allow free movement of the tongue and this restriction in tongue movement results in feeding difficulty. The lingual frenulum is formed of a fold in the mucosa and fascia which extends across the floor of and attaches to the underside of the tongue (Mills, et al, 2019). It is important to know that a lingual frenulum is normal anatomy and provided it is long, elastic and/or not attached in a way that restricts tongue movement it is not a tongue-tie. A study of 200 newborns on Israel in 2014 (Haham, et al, 2014) found that 199 of those babies had a lingual frenulum but only six had a tongue-tie requiring division for feeding difficulties.
So, when people describe a tongue-tie as ‘posterior’ what do they mean? The definition of a ‘posterior’ tongue-tie is not clearly defined but the use of the terms ‘anterior’ and ‘posterior’ describe the appearance of the frenulum.
‘Anterior’ frenula are attached at or close to the tip of the tongue with the lower part of the frenulum attaching onto the lower gum ridge or just below it. These tongue-ties are quite visually obvious when the tongue is.
Image below:
These parents often do not have a clue what this terminology means as no one has explained it to them. But they are sometimes given the impression division of this type of tongue-tie is complicated and risky. So, this blog will seek to address this.
A tongue-tie occurs when the lingual frenulum is too short, and/or tight and/or is attached to close to the tip of the tongue to allow free movement of the tongue and this restriction in tongue movement results in feeding difficulty. The lingual frenulum is formed of a fold in the mucosa and fascia which extends across the floor of and attaches to the underside of the tongue (Mills, et al, 2019). It is important to know that a lingual frenulum is normal anatomy and provided it is long, elastic and/or not attached in a way that restricts tongue movement it is not a tongue-tie. A study of 200 newborns on Israel in 2014 (Haham, et al, 2014) found that 199 of those babies had a lingual frenulum but only six had a tongue-tie requiring division for feeding difficulties.
So, when people describe a tongue-tie as ‘posterior’ what do they mean? The definition of a ‘posterior’ tongue-tie is not clearly defined but the use of the terms ‘anterior’ and ‘posterior’ describe the appearance of the frenulum.
‘Anterior’ frenula are attached at or close to the tip of the tongue with the lower part of the frenulum attaching onto the lower gum ridge or just below it. These tongue-ties are quite visually obvious when the tongue is.
Image below:
Coryllos/Watson Genna Typing System (2004)
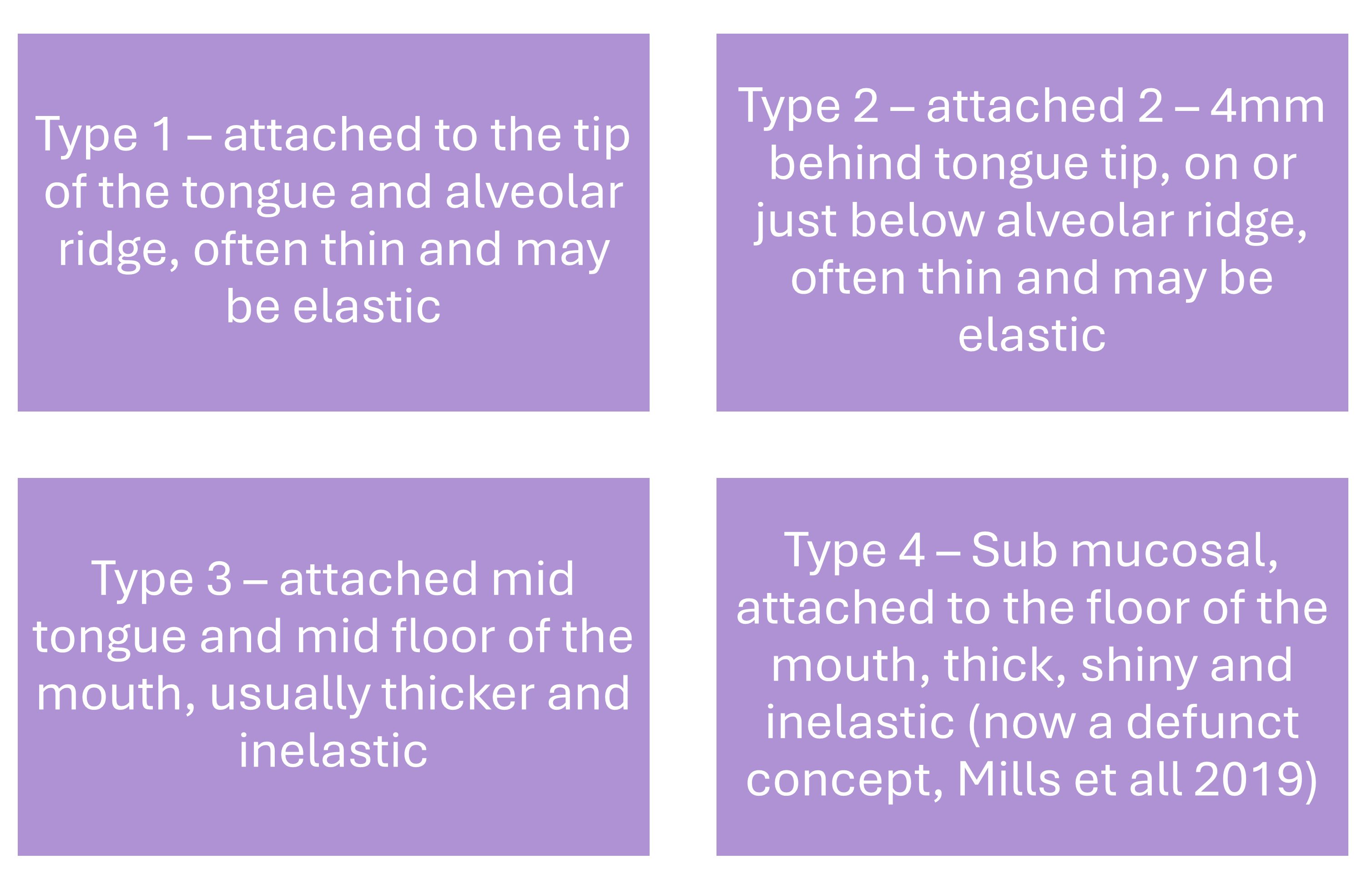

It is important to understand that the tongue and frenulum are not isolated structures. They are connected to several muscles and fascia. Tension and strain in these structures will influence tongue movement and feeding. Furthermore, into the genioglossus muscle does carry a higher risk of bleeding, damage to the lingual nerve and when we were doing these procedures there were higher rates of recurrence observed. When I trained to do division at Southampton in 2011 Carolyn Westcott told me 40% of the babies, they saw who had had division for ‘sub-mucosal’ tongue-tie returned for second divisions. A recent annual audit by the Association of Tongue-tie Practitioners have found the rate of second divisions to be 2-2.5% overall for all types of tongue-tie. So, 40% is very high indeed.
A lot of clinicians regarded these sub-mucosal tongue-ties as the true ‘posterior’ tongue-ties and would refer to all others as ‘anterior.’ The terms ‘sub-mucosal’ and ‘posterior’ have been used interchangeably to describe this type of tongue-tie.
In some babies where there is no apparent frenulum one will emerge after some bodywork to release the fascia. in these cases if the bodywork has not helped to resolve the feeding difficulty then division of the emerged frenulum can be considered after reassessment of tongue function and feeding.
Like every aspect of tongue-tie in babies there is controversy over how we describe and classify a tongue-tie. But the bottom line if someone is saying the tongue-tie is ‘posterior’ it just means the frenulum to attached further back along the underside of the tongue. Anyone still talking about sub-mucosal ties considering the research from New Zealand, which is now 5 years old, needs to update their knowledge.
So, my answer to the question ‘do I cut posterior tongue-ties’ is that I divide all types of tongue-tie. But I look beyond the frenulum and consider how other structures connected to the tongue and frenulum may also be restricting tongue movement and all the factors that may be impacting feeding to optimise feeding outcomes. It must be remembered that there is no evidence that simply dividing a tongue-tie will improve breastfeeding duration. A holistic approach is required and skilled, robust assessment pre- division and support after division are crucial. It is vital that whatever you are told about your baby’s tongue-tie you see a skilled and experienced tongue-tie practitioner. Preferably one who is an IBCLC.
In some babies where there is no apparent frenulum one will emerge after some bodywork to release the fascia. in these cases if the bodywork has not helped to resolve the feeding difficulty then division of the emerged frenulum can be considered after reassessment of tongue function and feeding.
Like every aspect of tongue-tie in babies there is controversy over how we describe and classify a tongue-tie. But the bottom line if someone is saying the tongue-tie is ‘posterior’ it just means the frenulum to attached further back along the underside of the tongue. Anyone still talking about sub-mucosal ties considering the research from New Zealand, which is now 5 years old, needs to update their knowledge.
So, my answer to the question ‘do I cut posterior tongue-ties’ is that I divide all types of tongue-tie. But I look beyond the frenulum and consider how other structures connected to the tongue and frenulum may also be restricting tongue movement and all the factors that may be impacting feeding to optimise feeding outcomes. It must be remembered that there is no evidence that simply dividing a tongue-tie will improve breastfeeding duration. A holistic approach is required and skilled, robust assessment pre- division and support after division are crucial. It is vital that whatever you are told about your baby’s tongue-tie you see a skilled and experienced tongue-tie practitioner. Preferably one who is an IBCLC.

Copyright © 2025
Created with